 The Problem, The Cause, The Solution
The Problem, The Cause, The Solution
THE PROBLEM
Firefighters are fit and follow a vigorous life-style, yet they experience more heart attacks compared to the general population. Cardiovascular disease (CVD) has been reported to be highly prevalent in firefighters as illustrated by the Toronto FD study in which the CVD mortality ratio for firefighters, aged 45-49 years, was 1.7 time higher when compared to non-firefighters. The Centers for Disease Control confirms that among career firefighters, sudden cardiac death and asphyxiation are the leading causes of death and FEMA states that coronary heart disease (CHD) is the greatest health risk to firefighters.
Even in young, fit firefighters, changes in blood chemistry after just 18 minutes of suppression activity can lead to a sudden cardiac event
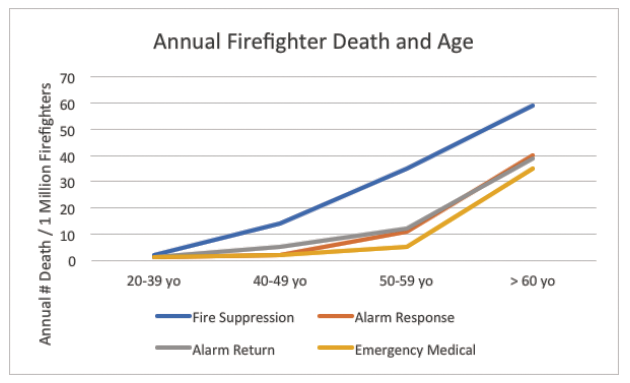
The odds of a CVD event in firefighters appears to be linked to specific job activities. Compared to non-emergency duties, fire suppression and alarm response carried significantly higher risks of CHD death. The conclusion is that most firefighter on-duty CHD fatalities are work precipitated with no prior warning.
A medical article in 2007 highlighted the health problem in firefighters and came to three key conclusions. First, since the 1970’s, sudden coronary death accounted for 45% of all on-duty firefighter deaths. Second, the relative risk for sudden coronary death during fire suppression activity is 10 -100 times greater than during non-emergency duties. Third, and perhaps most important, on-duty sudden coronary death occurs most in firefighters with existing CHD that they were not aware of. Thus, the PROBLEM is an extremely high CHD risk in firefighters linked to job activities which are most threatening in firefighters with undiagnosed CHD.
THE REASON
The cause of this high incidence of CHD in firefighters was investigated in the National Firefighter Heart Disease Prevention Study (FEMA-2006). In this study, 1/3 of “healthy” firefighters, over the age of 40 years, had coronary artery computerized tomography (cardiac CT) evidence of previously undiagnosed heart disease. In short, a cardiac CT scan showing coronary artery calcium diagnosed the presence of subclinical CHD. It is important to note that while age was a bit higher in the cardiac CT positive firefighters (not unexpected), the standard screening heart disease risk factors of high blood cholesterol, high triglycerides, or low HDL cholesterol did not identify the firefighters vulnerable to a heart attack.
Traditionally exercise stress tests have been utilized to screen for CHD but these tests do not detect disease until it is well advanced and obstructs approximately 70% or more of the coronary artery. Most heart attacks are the result of a non-obstructive plaque that suddenly ruptures and blocks the artery. The need is for a test that can identify firefighters who are “healthy” yet have undetected heart disease. One non-invasive test, that costs around $100, and has less radiation exposure than a chest X-ray, is a cardiac CT scan. The LA County Firefighter CAC study revealed that compared to non-firefighters, firefighters have significantly higher CAC scores and had three coronary arteries involved compared to one in the non-firefighter group. Thus, one REASON for the high rate of heart attacks in firefighters is the high level of undetected CHD.
 The metabolic cause of this high incidence of CAC scores and CVD risk in firefighters has been unclear but the Firefighter Heart Disease Prevention Study has shed light on how to identify the firefighter vulnerable to a heart attack. It was reported that the prevalence of obesity, elevated blood cholesterol, and elevated blood pressure were higher than the general population. However, in the FEMA study, traditional risk factors did a poor job of identifying the CHD vulnerable firefighter and non-traditional risk factors were better (Table 1). Measures of the metabolic syndrome and insulin resistance were the strongest predictors of CAC score, and measures of both blood and genetic markers of a prothrombotic state were associated with higher CAC scores. It was concluded that aspects of insulin resistance and thrombosis were related to CHD risk among firefighters.
The metabolic cause of this high incidence of CAC scores and CVD risk in firefighters has been unclear but the Firefighter Heart Disease Prevention Study has shed light on how to identify the firefighter vulnerable to a heart attack. It was reported that the prevalence of obesity, elevated blood cholesterol, and elevated blood pressure were higher than the general population. However, in the FEMA study, traditional risk factors did a poor job of identifying the CHD vulnerable firefighter and non-traditional risk factors were better (Table 1). Measures of the metabolic syndrome and insulin resistance were the strongest predictors of CAC score, and measures of both blood and genetic markers of a prothrombotic state were associated with higher CAC scores. It was concluded that aspects of insulin resistance and thrombosis were related to CHD risk among firefighters.
Metabolic Syndrome. The metabolic syndrome is a grouping of risk factors that include insulin resistance, abdominal obesity, elevated blood trigylcerides and low blood HDL-cholesterol. Along with excess body fat (but not always) is the condition of insulin resistance which can be viewed as stressing the pancreas and is a precursor of type II diabetes. Elevated fasting blood insulin levels is one way to detect insulin resistance.
Thrombosis. An important component of the metabolic syndrome is dysfunction within the blood clotting and un-clotting system. This dysfunction includes aspects of both fibrinolysis (a break-down of fibrin) and thrombosis.
Genetics. Inheritance of a slight to moderate genetic proclivity to thrombosis may contribute to the association of firefighter job activity and CHD events. The FEMA study reported that firefighters with a positive CAC test had significantly higher plasminogen, fibrinogen, PAI-I, homocysteine and Lp(a) levels compared to firefighters who did not have a positive CAC test. Each of these measurements was not significant enough to be meaningful in a normal work environment but, in the setting of high intensity firefighter activities could collectively contribute to sudden cardiovascular events. The FEMA study analyzed 1,000,000 single nucleotide polymorphisms in each firefighter and found that several blood and genetic markers reflecting a proclivity to thrombosis were significantly higher in firefighters with a positive CAC score. An investigation at the Illinois Fire Service Institute reported that blood from firefighters, before and after different job assignments, revealed a 15% reduction in plasma volume after 18 minutes, which can lead to an occlusive thrombus and a sudden cardiac event.
Treatment of the metabolic syndrome can be successful and relatively low cost. In a study of first responders in Boston and Phoenix, a combination of online tools for tracking and managing diet, exercise, and weight with telephonic health coaching resulted in a significant improvement of Metabolic Syndrome components.
THE SOLUTION
The solution involves 1) identification of the vulnerable firefighter, 2) diagnosing the cause of CHD in the individual firefighter, and 3) designing an effective and individualized treatment program. For the firefighter less than 40 years of age, the blood tests take on added importance since he/she may have the metabolic stew that slowly contributes to CHD but has not yet had the time to result in coronary artery calcification. Firefighters over the age of 40 are more likely to reveal coronary artery calcification which identifies a firefighter in which coronary artery disease is already present and thus a higher risk for a heart attack.
Recently, firefighters in Carmel, Monterey, Seaside and Bozeman, MT have been screened with both blood and CAC tests. Consistently, approximately 1/3 of the firefighters have been found to have subclinical coronary heart disease that they were unaware of. The risk markers found in the FEMA study are also consistently associated with a positive CAC score as well as a relatively new risk factor. This new risk factor is the blood fish oil (fatty acids) levels commonly known as EPA and DHA. The average percent of blood fatty acids that are the combination of EPA+DHA in the American population is about 4%. In the firefighter population it was found to be 2.8%. This can be improved through dietary change.
Summary:
Firefighters have a much higher risk of heart attack and coronary death compared to the non-firefighter population. We now know many of the underlying causes, and treatment is often not difficult. However, the treatment must be matched to the individual cause of coronary heart disease and the same treatment is not necessarily the best treatment for everyone.
By H. Robert Superko, MD, FACC, FAHA, FASPC; Richard E. George, LAFD retired; Spencer Reade, Monterey Co. FD; Brenda Garrett, RN and Basil Margolis, MD, FACC, Emory University
